
MH Crisis. Have you done all that can be done to be prepared?
- Elite Accreditation Consultants
- May 25
- 3 min read

No matter how often you work to prepare your staff, a MH crisis is going to be exceptionally hard at the moment of an event. The best thing you can do is to ensure the staff are educated, trained, and prepared. We have provided you some helpful tips at ensuring your readiness:
**MALIGNANT HYPERTHERMIA (MH)
EMERGENCY RESPONSE & COMPLIANCE MANUAL** (ASC/OBL/Procedure Centers)
TABLE OF CONTENTS
Policy & Purpose
Scope
Definitions
MH Triggering Agents
Early Recognition Criteria
Emergency Response Protocol (Step-by-Step)
Dantrolene Preparation & Dosing Guide
MH Cart Requirements & Inventory Log
Staff Roles During MH Event
Transfer & Escalation Procedures
Post-Event Management
Staff Training & Drill Requirements
Documentation Requirements
Quality Assurance & QAPI Integration
Forms & Logs (Fillable Templates)
1. POLICY & PURPOSE
The facility maintains a fully equipped malignant hyperthermia (MH) response system to ensure rapid identification and treatment of MH events in accordance with:
CMS Conditions for Coverage (ASC)
The Joint Commission standards
American Society of Anesthesiologists guidelines
Malignant Hyperthermia Association of the United States recommendations
2. SCOPE
Applies to:
All anesthesia providers
Registered nurses
Surgical technologists
Medical staff
Emergency response personnel
3. DEFINITIONS
Malignant Hyperthermia (MH):A pharmacogenetic disorder triggered by certain anesthetic agents causing uncontrolled skeletal muscle metabolism.
4. MH TRIGGERING AGENTS
Known Triggers
Volatile anesthetics:
Sevoflurane
Desflurane
Isoflurane
Succinylcholine
Non-Triggering (Safe) Agents
Propofol
Ketamine
Midazolam
Fentanyl
Rocuronium / Vecuronium
Local anesthetics
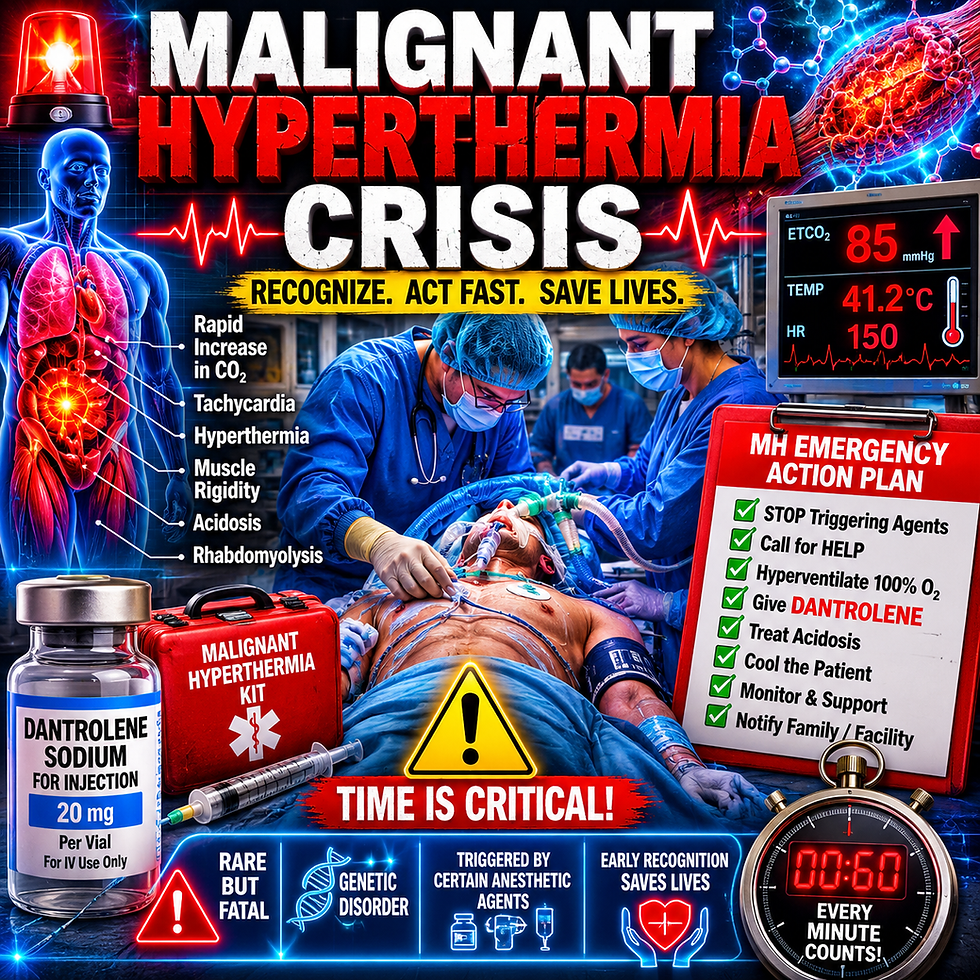
5. EARLY RECOGNITION CRITERIA
MOST IMPORTANT (EARLY SIGNS):
Rapid rise in ETCO₂
Tachycardia
Muscle rigidity (especially jaw)
LATE SIGNS:
Hyperthermia
Dark urine (myoglobinuria)
Acidosis
Hyperkalemia
6. EMERGENCY RESPONSE PROTOCOL
IMMEDIATE ACTIONS (0–5 MINUTES)
STOP triggering agents immediately
Call MH CODE
Hyperventilate with 100% O₂ at high flow
Discontinue volatile anesthetics
Activate MH cart
TREATMENT ACTIONS
Administer Dantrolene immediately
Initiate active cooling:
Ice packs (groin, axilla, neck)
Cold IV saline
Monitor:
ETCO₂
Core temperature
ABGs
Electrolytes
7. DANTROLENE DOSING GUIDE
Initial Dose:
2.5 mg/kg IV push
Repeat:
Every 5 minutes until symptoms controlled
Max cumulative: 10 mg/kg (or higher per MD)
RECONSTITUTION
Dantrium/Revonto: 20 mg vial + 60 mL sterile water
Ryanodex: 250 mg vial + 5 mL sterile water
👉 Ryanodex preferred for rapid response
8. MH CART REQUIREMENTS
MANDATORY CONTENTS
Dantrolene (minimum supply per guidelines)
Sterile water for injection
Syringes (large volume)
Cooling supplies
Sodium bicarbonate
Insulin + Dextrose
Calcium chloride
Antiarrhythmics
Foley catheter kit
Temperature probes
MH CART LOG (Sample)
Date | Checked By | Dantrolene Count | Expiration Verified | Supplies Complete | Notes |
9. STAFF ROLES DURING MH EVENT
Anesthesia Provider
Leads response
Administers dantrolene
Circulating Nurse
Activates MH cart
Documents timeline
Scrub Tech
Assists with supplies
Runner
Mixes dantrolene
Retrieves additional supplies
10. TRANSFER & ESCALATION
Stabilize patient
Arrange emergency transfer to higher level of care
Notify receiving hospital of MH event
11. POST-EVENT MANAGEMENT
ICU monitoring (24–48 hrs)
Monitor for recurrence
Document fully
Report to:
Malignant Hyperthermia Association of the United States registry
12. STAFF TRAINING & DRILLS
REQUIREMENTS:
Annual MH competency validation
Mock drill at least annually (best practice: quarterly)
DRILL DOCUMENTATION LOG
Date | Scenario | Staff Involved | Response Time | Deficiencies | Action Plan |
13. DOCUMENTATION REQUIREMENTS
Event timeline
Medications administered
Vital signs
Transfer details
Incident report
14. QUALITY ASSURANCE (QAPI)
Include:
Drill performance review
Cart audit compliance
Staff competency tracking
Incident trending
15. FORMS & TEMPLATES (READY TO USE)
A. MH EVENT FLOW SHEET
Time-based intervention tracking
Medication log
Vital signs grid
B. MH CRASH CART CHECKLIST
Daily / weekly verification
Expiration tracking
C. STAFF COMPETENCY CHECKLIST
Recognition of MH
Dantrolene preparation
Emergency response steps
D. POST-EVENT REVIEW FORM
Root cause analysis
Performance scoring
Corrective actions


Comments